![]()
read more

The possibilities in healthcare are becoming increasingly greater. New technology and better treatments contribute to a better and longer life. Innovative medicines increasingly focus on a specific disorder or small group of patients. It is then important to ensure that new medicines reach the patient. Access to medicines depends on availability, procedures and affordability.
 Access to medicines depends primarily on the admission of medicines into the market and into health insurance. Patients have access to a new medicine if it has been admitted to the market by the European Medicines Agency (EMA). It is then up to the Minister of Health, Welfare and Sport and health insurers to also admit medicines to the health insurance package. As of that moment, physicians can also actually prescribe these medicines.
Access to medicines depends primarily on the admission of medicines into the market and into health insurance. Patients have access to a new medicine if it has been admitted to the market by the European Medicines Agency (EMA). It is then up to the Minister of Health, Welfare and Sport and health insurers to also admit medicines to the health insurance package. As of that moment, physicians can also actually prescribe these medicines.
The total expenditures on medicines amounted to € 6.2 billion in 2020, excluding pharmacy remuneration. That is 8.3% of the total healthcare budget. Compared to other countries in Europe, the Dutch spend little on medicines. Only residents of Luxembourg, Ireland and Denmark spend less.
Expenditures on medicines are an investment in healthcare and health and therefore in the economy. We save healthcare costs and contribute to the health of Dutch people so that they can actively participate in society.
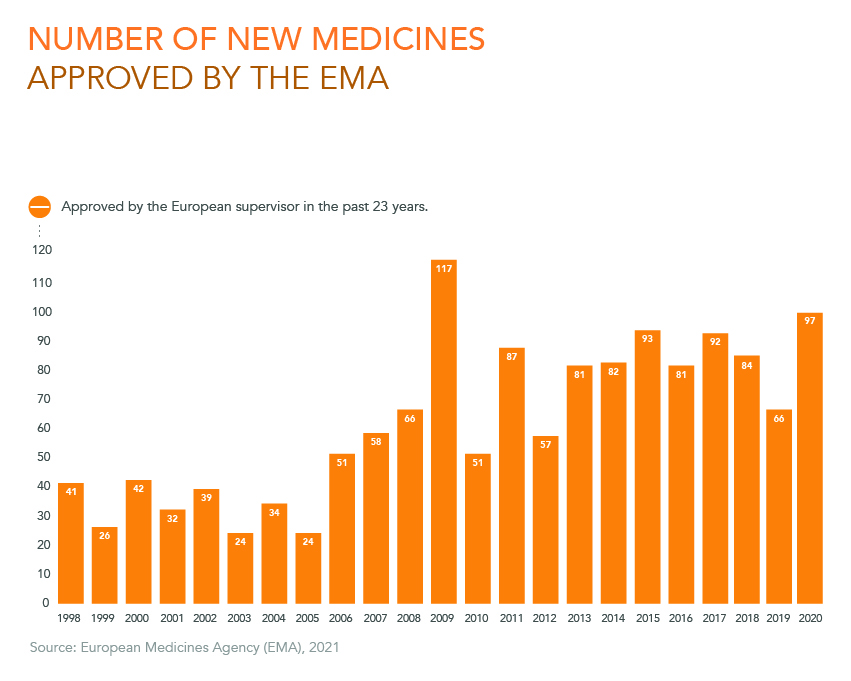
Source: European Medicines Agency (EMA), 2021
The number of medicines approved for the European market has increased in the past 23 years. The European Medicines Agency (EMA) approved 97 new medicines in 2020. In 39 of these cases, the medicine was an innovative drug with a new active ingredient.
The EMA assesses new medicines for efficacy and safety. The EMA has been located in Amsterdam since 2019. The arrival of the EMA is great news for the Netherlands and makes it attractive for companies to establish themselves in the Netherlands. In this way, the EMA acts as a magnet for innovation in the Netherlands.
More medicines continue to appear for the approximately 7,000 rare diseases. These medicines are also called orphan drugs. A disease is considered rare when fewer than 1 in 2,000 people have the disease. In the last 20 years, the EMA approved 191 drugs for more than 100 rare diseases. The number of clinical studies into rare diseases increased by 88% between 2006 and 2016. This has resulted in an increasing number of orphan drugs for the patient.
With these numbers, Europe is the worldwide leader in clinical research into orphan medicines. Research in this category faces challenges. It involves small groups of patients, which makes it more difficult to conduct a representative study. In addition, the investments are relatively high. Nevertheless, this research is highly necessary. In 1999, the European Union adopted a special regulation in order to stimulate the development of orphan medicines. That policy is yielding positive results.
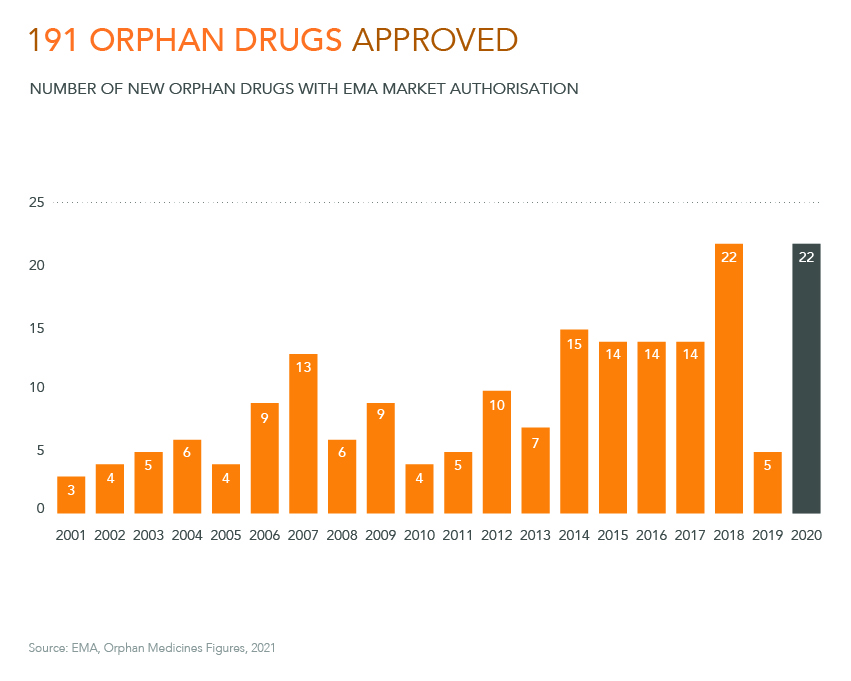
Source: EMA, Orphan Medicines Figures, 2021

Source: C. Uyl-de Groot, R. Heine, M. Krol & J. Verweij, Unequal access to Newly Registered Cancer Drugs Leads to Potential Loss of Life-Years in Europe, 2020
A pharmaceutical company cannot sell a new medicine until it has been registered. Registration can be done at European level via the European Medicines Agency (EMA). In the US, registration is done via the Food and Drug Administration (FDA). They assess the new medicine for efficacy and safety.
On average, the assessment of new medicines against cancer in E urope takes 378 days. In the US, new medicines against cancer are assessed faster, on average in 181 days.
When the medicine has been registered with the EMA or the CBG (College ter Beoordeling van Geneesmiddelen [Medicines Evaluation Board]), it will not be automatically reimbursed by healthcare insurers. Medicines must first still be admitted to health insurance. This concerns the Minister of Health, Welfare and Sport (VWS) or healthcare insurers. Medicines are tested to determine whether they meet the state of science and practice. Medicines are then given a place in physician treatment guidelines. Meanwhile, manufacturers negotiate with the Minister, healthcare insurers or hospitals about the price of the medicine, but also about, for example, appropriate use and the use of medicines in specialised centres.
In the Netherlands, it takes an average of 128 days after EMA registration before a new medicine against cancer is available to the patient. That puts us in ninth place in Europe.
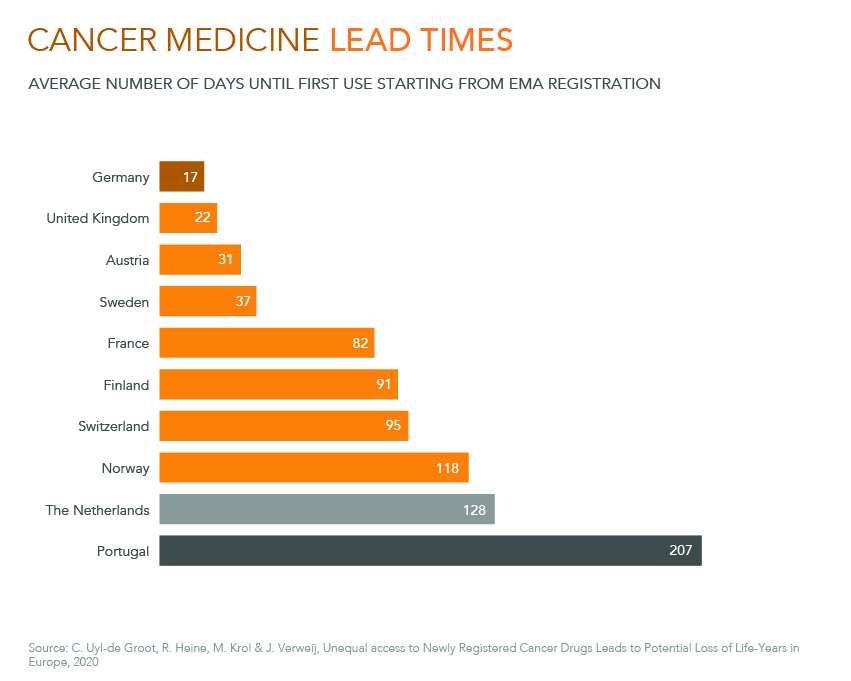
Source: C. Uyl-de Groot, R. Heine, M. Krol & J. Verweij, Unequal access to Newly Registered Cancer Drugs Leads to Potential Loss of Life-Years in Europe, 2020

Source: BSHealth, 2019: Toegankelijkheid van innovatieve geneesmiddelen
When a new medicine is prescribed in hospitals, Dutch patients will be automatically reimbursed from their basic insurance. This still does not mean that all patients receive the medicine immediately. When a medicine costs society more than € 40 million per year in total, it is placed in the so-called “lock”. This also occurs when the medicine costs more than € 50,000 per patient and a total of € 10 million per year. As long as a medicine is in the lock, which is an average of 345 days, it is not available for the patient. The lock often results in a financial arrangement between the government and a pharmaceutical company.
In addition, physicians often only prescribe a medicine when it has separate financing, which is called an add-on. Even for drugs that have not been placed in the lock, it takes 149 days on average before physicians will prescribe the new medicine. It is very important to reduce these periods for the patient. For this purpose, consultation is necessary between all parties involved.
Medicines that get to the patient via the public pharmacy will not be automatically reimbursed from the basic insurance. A drug company must apply for reimbursement through the Geneesmiddelen Vergoeding Systeem (GVS) [Medicines Reimbursement System]. This application is submitted to the Minister of Medical Care, who requests a recommendation from the National Healthcare Institute. Based on this recommendation, these medicines will be placed in a cluster with a reimbursement limit (list 1a) or put on a separate list without limit (1b). These procedures last on average 365 days (1a) and 325 days (1b).
The Minister sometimes still negotiates with the pharmaceutical company about a financial arrangement for expensive medicines. Just as with the lock, this occurs when the total cost is more than € 40 million per year or more than € 50,000 per patient and more than € 10 million in total. This takes an average of 237 days. Proper consultation is also necessary here in order to be able to help the patient faster.
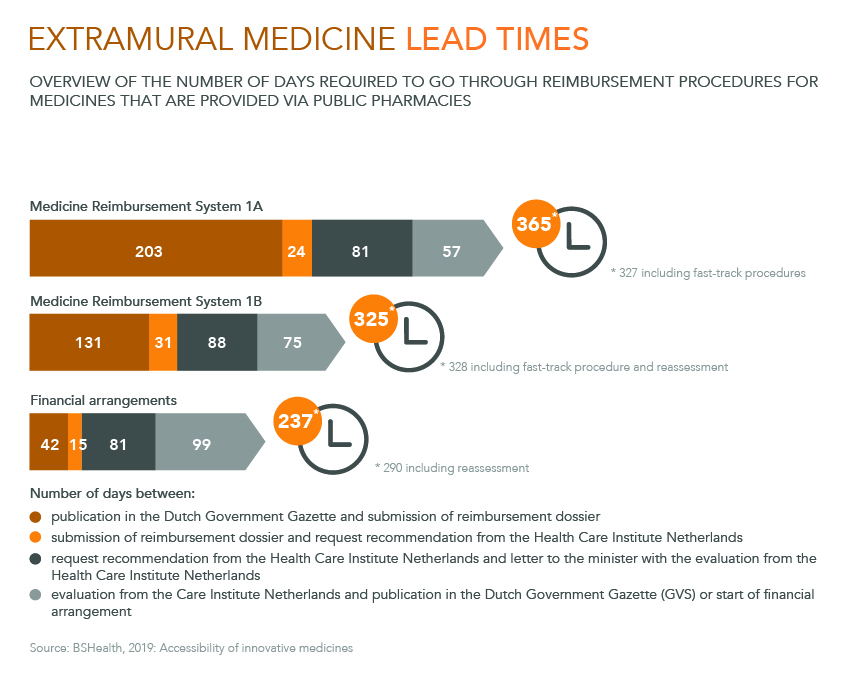
Source: BSHealth, 2019: Accessibility of innovative medicines

Source: 2021 VWS (Volksgezondheid, Welzijn en Sport) [Health, Welfare and Sport]) Budget; SFK, Data and Facts, 2020; GIPdata, 2020; Axon Healthcare, 2020
The healthcare expenditures that count towards the Budgetary Healthcare Framework consist of the Healthcare Insurance Act, the Long-Term Care Act and other expenditures.
Costs for medicines are covered under the Healthcare Insurance Act. A distinction is made here between medicines that are dispensed inside and outside of hospitals. The medicines that are provided within hospitals are intramural medicines. This group falls in the Medical Specialist healthcare category. The medicines that are provided outside of hospitals are extramural. This group falls in the pharmaceutical care category. The expenditures on intramural and extramural medicines in 2019 amounted to € 6.2 billion.
The expenditures in this overview are based on the medicine list prices. In practice, the costs of specialist medicines are lower. The reason for this is because insurers, hospitals, pharmacies and sometimes the government itself negotiate with the manufacturer about the medicine’s price. The result from these negotiations is only partially public.
In the Netherlands, we spend relatively little on medicines compared to other wealthy countries. Compared to the Gross Domestic Product (GDP), expenditures on medicines and medical devices in the Netherlands is only 1.24%. The average in the European Union is 1.81%.
However, in the Netherlands, we pay almost as much for total healthcare as other wealthy countries. This is due to the fact that the Netherlands spends a relatively large amount on hospital and long-term care.
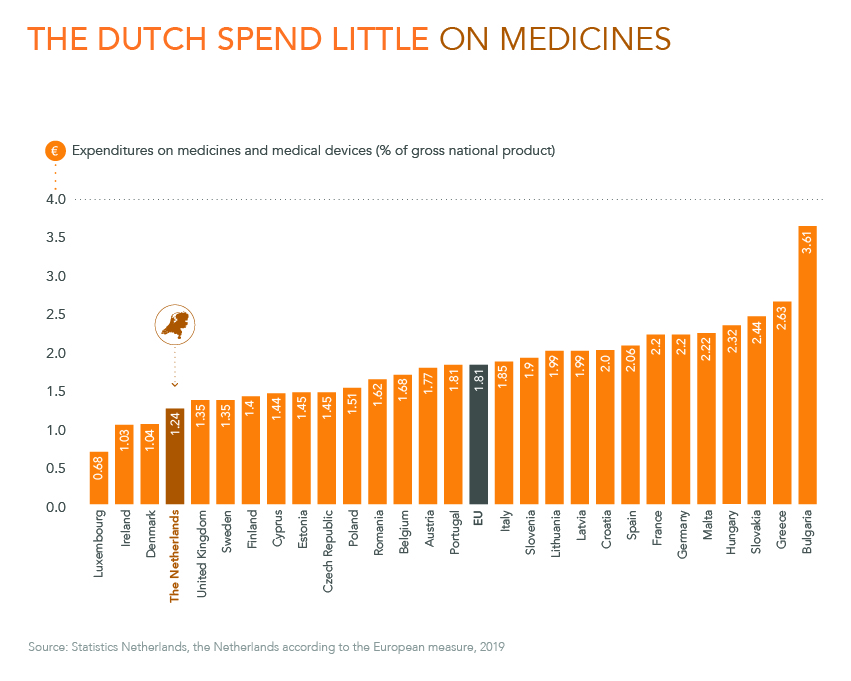
Source: Statistics Netherlands, the Netherlands according to the European measure, 2019
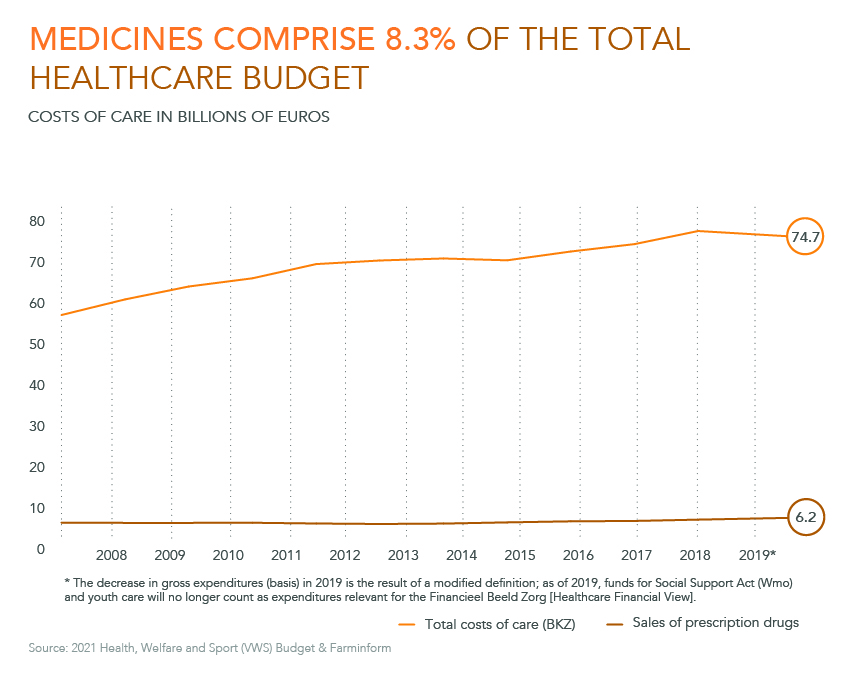
Source: 2021 Health, Welfare and Sport (VWS) Budget & Farminform
Over the past decade, the total government expenditures on healthcare has increased from € 56 to € 74.7 billion. The expenditures for medicines increased to € 6.2 billion, excluding the pharmacy remuneration. The share of medicines in the healthcare budget decreased in this period from 8.9% to 8.3%.
Total market sales of prescription medicines have risen in the past ten years. The changes mainly involve shifts: the sales of medicines provided in the hospital (intramural) increased to € 3.0 billion in 2019. This regards € 2.4 billion in specialist medicines and € 0.6 billion for other medicines. The expenditures on medicines provided by the public pharmacy (extramural) have increased since 2015 from € 3.1 billion to € 3.2 billion.
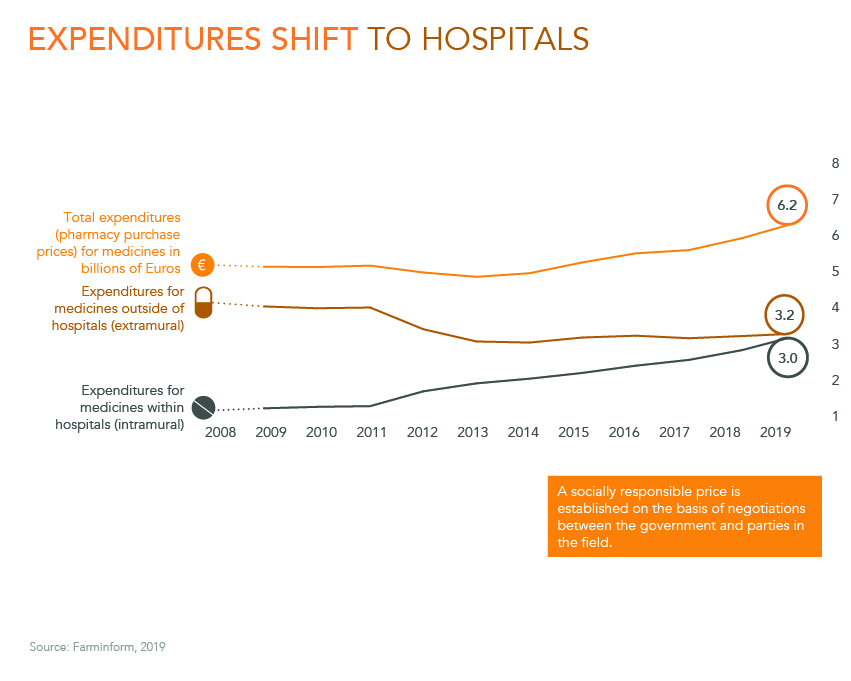
Source: Farminform, 2019

Source: Deloitte, Source: GIP database, Dec. 2020
In recent years, the costs of medicines per hospital patient have decreased by 5% per year from an average of almost € 10,000 per patient to about € 8,100. The fact that the hospital expenditures on medicines are increasing is mainly due to a growth in the number of patients. The number of patients using hospital medicines increased by 14% per year between 2015 and 2019. It should be noted here that the increase in the number of users has been strongly influenced by a number of medicines.
Consumer prices have increased in the past 20 years. Prices, for example, of housing and transportation, increased an average of 2% per year. Medicine prices increased 0.5% per year
in the same 20 years. The price index of pharmaceutical products in 2019 is 116. This is almost the same as the 2007 level, when the price index was 114.
Total expenditure on medicines increased slightly more than this percentage because the total medicine use increased. And that is due to the fact that more Dutch use medicines (especially due to ageing) and the use per person is growing.
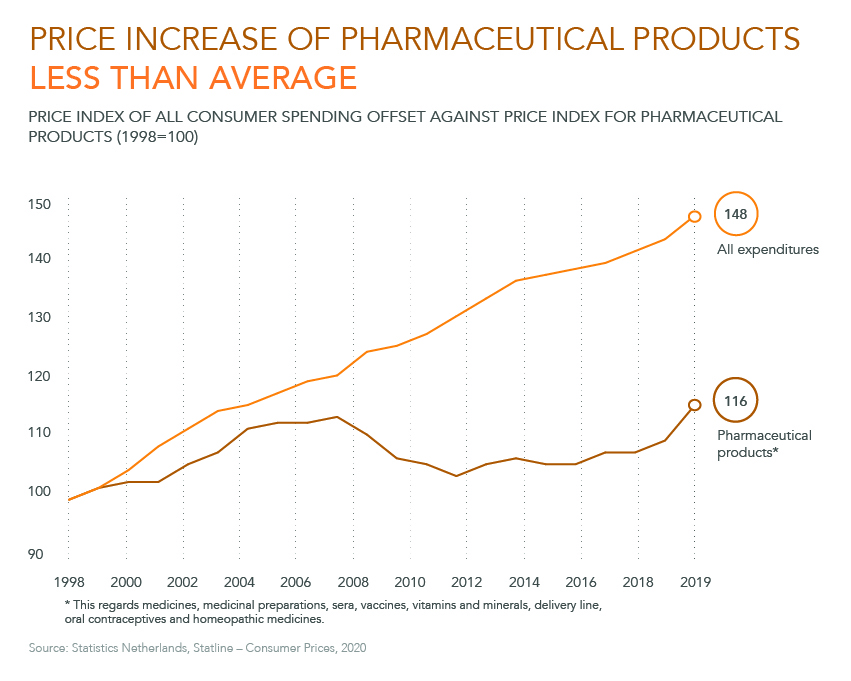
Source: Statistics Netherlands, Statline – Consumer Prices, 2020
Source: FarmInform, 2018
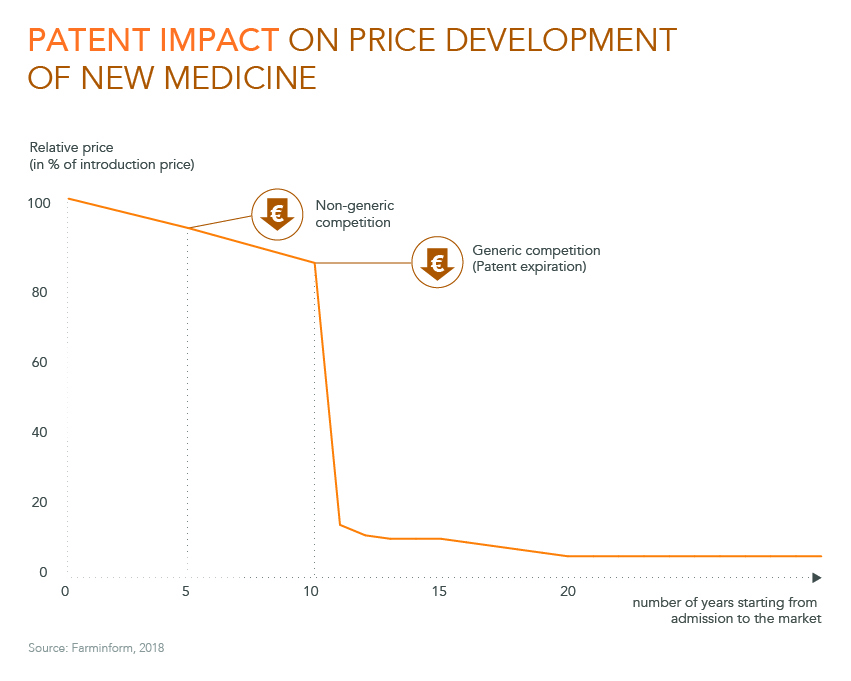
When determining the impact of a medicine on the healthcare budget, it is often only viewed at the time when the drug costs the most. But the expenditure on a medicine is never stable. Because other companies also make medicines for the same disease, competition sets in. Changes in the determination of the maximum prices that are set by the Medicines Pricing Act (WGP) also result in changes in the expenditures on medicines.
When the patent on a medicine expires, other companies may replicate the medicine. As a result, the competition increases further, as a result of which prices decrease. The medicine is then available for a fraction of the original price. Patients can then profit from the innovation for decades to come.
Medicines are of essential value for people. For example, the life expectan cy with cancer has increased significantly over the past decades and HIV is no longer a death sentence. However, the pharmaceutical sector also adds value to society in many other ways . For example, medicines often prevent the need for other care, such as surgery, transplants and hospitalisations.
In addition, medicines prevent many costs that arise due to disability, for example, in the case of rheumatism, or absenteeism costs due to flu. In addition , the sector also provides a high level of economic value: it provides jobs, provides work to other sectors (for example, transport) and contributes to the growth of the Dutch economy. Therefore, society amply recovers its investment in the medicine sector.
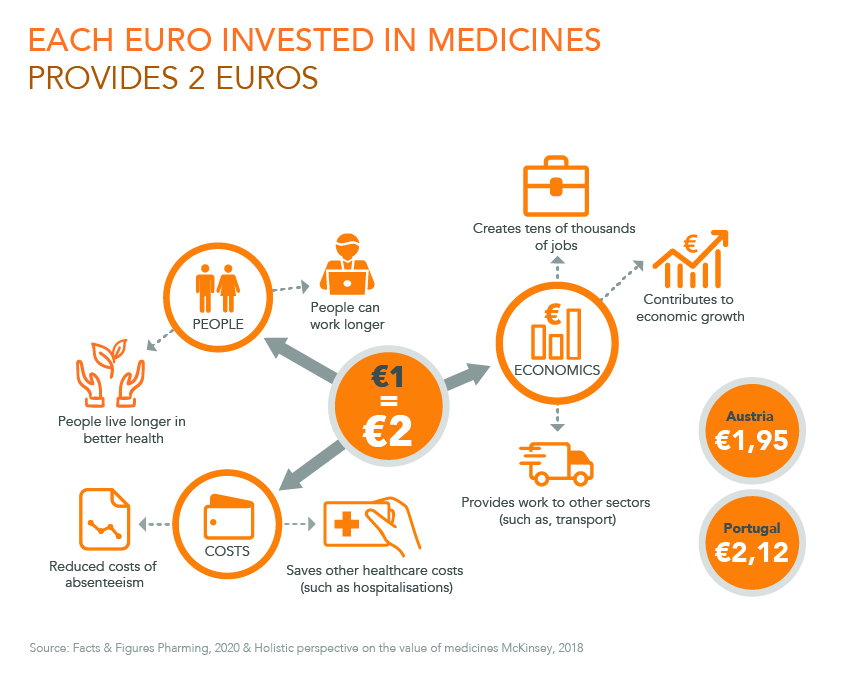
Bron: Facts & Figures Pharming, 2020 & Holistic perspective on the value of medicines McKinsey, 2018
Google+
Uw naam
Uw e-mail adres
Naam ontvanger
E-mail adres ontvanger
Uw bericht