read more


Many parties are involved in the development of new medicines. Drug companies pay almost three-quarters of all costs for drug research. The remaining costs are paid by the government, universities and non-profit organisations.
After discovering a potential medicine in the preclinical phase, pharmaceutical companies conduct studies in the clinical phase for years, with thousands of patients in various countries. When there is sufficient clarity about the effectiveness and side effects, this results in the registration of the new medicine. The total process of medicine development, including registration and reimbursement, takes on average approximately 12 years and costs 2.2 billion euros.
After the costly development, the patent allows a drug company an average of about 8 years to recoup the investments. After this, other companies are permitted to manufacture the product and the price often drops due to increased competition.
In 2018, more than 15,000 medicines were being developed worldwide. Drug companies work hard to find solutions for rare diseases, but also to find better treatments for many common disorders such as cancer and Alzheimer’s disease. More biological medicines and immuno-, cell and gene therapies have been introduced in recent years. The European Medicines Agency, EMA, granted registration to a total of 84 innovative medicines in 2018.
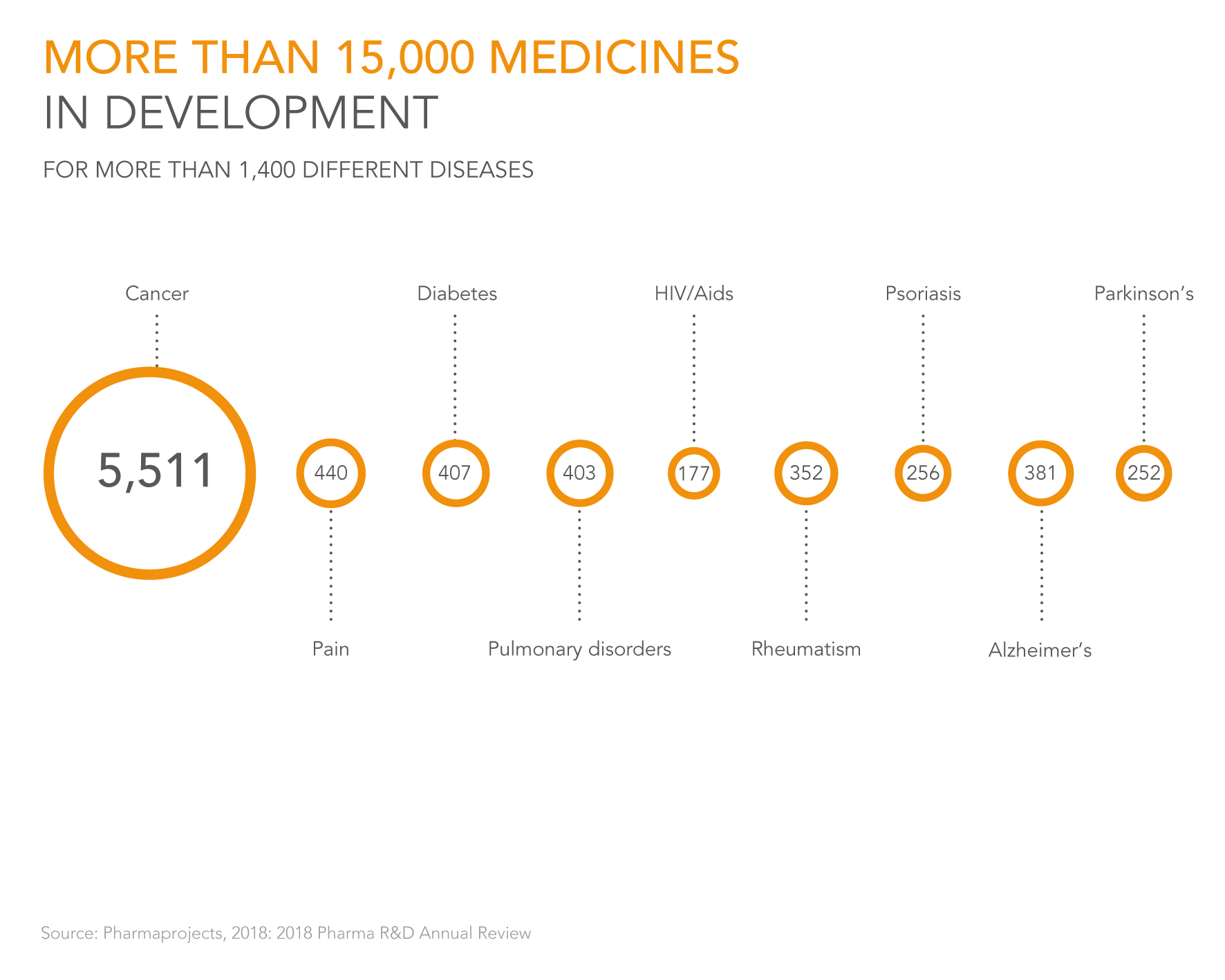
Source: Pharmaprojects, 2018: 2018 Pharma R&D Annual Review
Drug companies and universities worldwide are working hard on the discovery and development of new medicines. They do that in laboratories (in the preclinical phase) and with patient studies (the clinical phase). There were approximately 15,000 medicines in development in 2018. A Nature study conducted a few years ago made it clear that pharmaceutical companies discover 83% of all new medications.
More than one-third of all medicines in development are focused on cancer. It is also striking that for a disease like Alzheimer’s, for which there is still no medicine, there are many medicines in development: 381. Drug development is complex. As a result, only a very small percentage of the substances studied reach the finishing line.
It is becoming increasingly possible to use biomarkers, which are found in blood or tissue, to determine in advance whether a patient will benefit from a medicine. This makes it easier to immediately select the right medicine. Important for the patient, but also for the affordability of the system.
For 30% of the medicines that are already in the clinical phase, it is being investigated whether biomarkers can be developed as well. This proportion is even at 60% for the newer drugs, which are still in the preclinical phase.
Sometimes a medicine or treatment is even made fully customised, for example in cell or gene therapy. These are the so-called Advanced Therapy Medicinal Products (ATMPs).
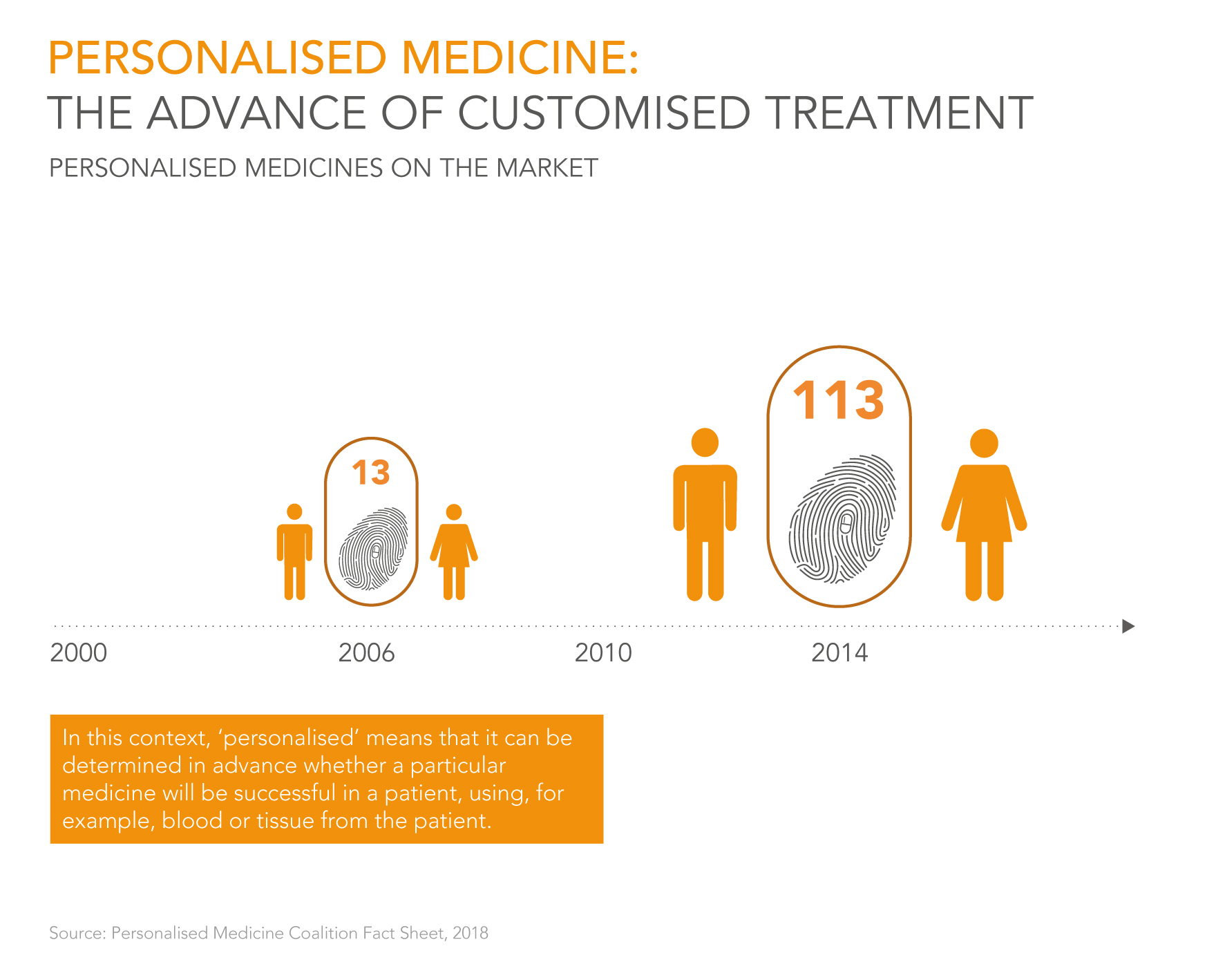
Source: Personalised Medicine Coalition Fact Sheet, 2018
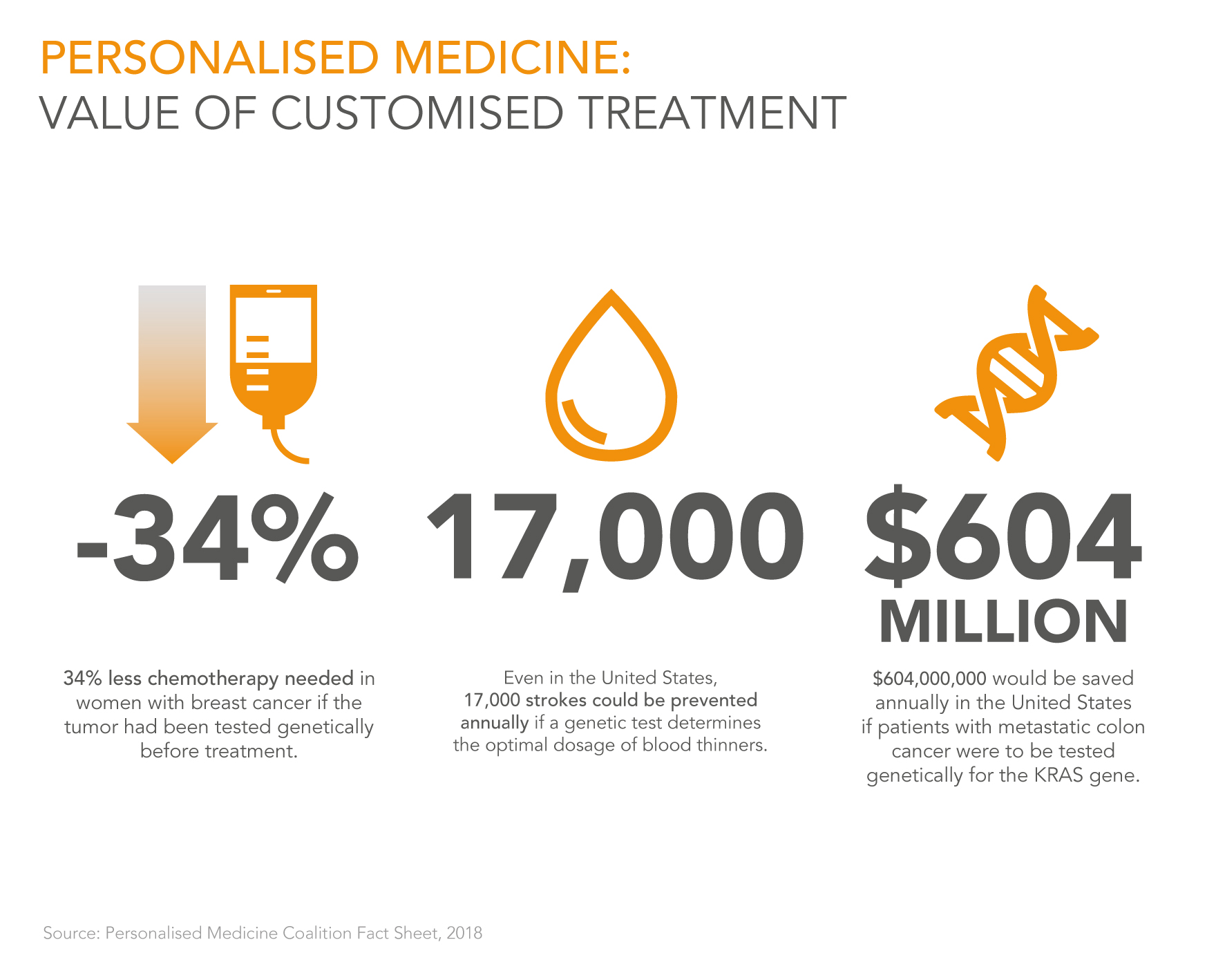
Source: Personalised Medicine Coalition Fact Sheet, 2018
Diseases can be better prevented with personalised treatment. An important tool for this purpose is genetic testing, with which it can be determined whether someone will develop a specific disease. Such predictions are mainly important for the patient’s health, because it is then possible to intervene early in many disorders. In addition, it can also save healthcare costs.
There are also other forms of personalised treatment. For example, it is becoming increasingly possible to predict via biomarkers, which are found in blood or tissue, whether a medicine will work for a specific patient. There has also been much progress made in recent years in immunotherapy, where the patient’s own immune system is reinforced.
Drug development is becoming increasingly more advanced. More often, it no longer concerns a pill, but rather a gene or cell therapy (ATMPs – Advanced Therapy Medicinal Products). This involves treating a patient’s genes or cells, inside or outside the body.
Sometimes, cells or genetic material from other people are also administered.
ATMPs often involve complex, expensive therapies. What is special about these treatments is that they are usually curative. That means that they only need to be administered once and, as a result, can be cost-effective (over time). Of the 1,003 ATMPs in development, more than half are focused on cancer.

Source: Alliance for Regenerative Medicine, 2018
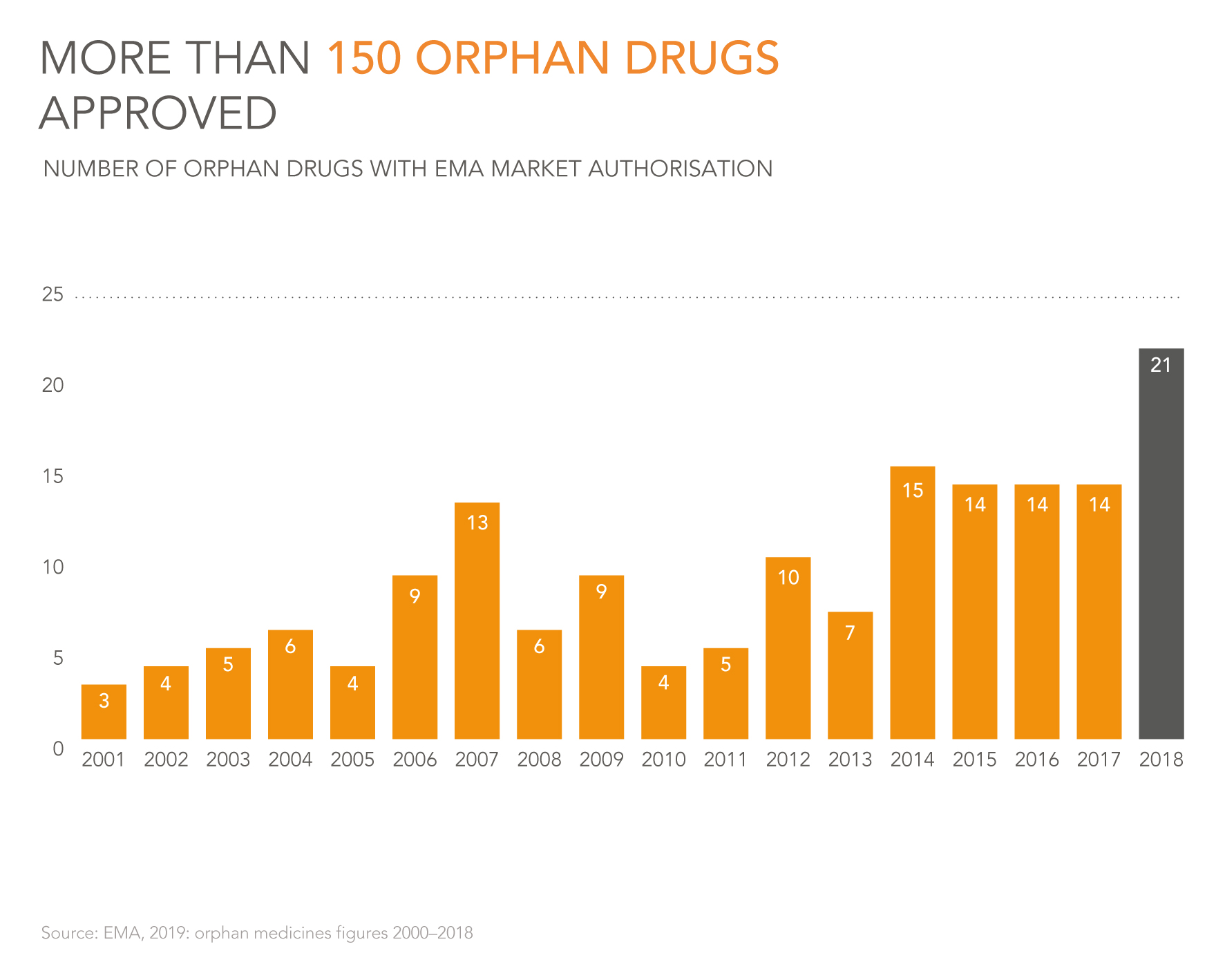
Source: EMA, 2019: orphan medicines figures 2000-2018
More medicines continue to be developed for the approximately 6,000 rare diseases. These medicines are also called orphan drugs. A disease is considered rare if fewer than one in 2,000 people have the disorder. In the last 20 years, the EMA approved 150 drugs for more than 90 rare diseases. The number of clinical studies into rare diseases increased by 88% between 2006 and 2016.
With these numbers, Europe is the worldwide leader in clinical research into orphan medicines. Research in this category is difficult. It involves small groups of patients, which makes it more difficult to conduct a representative study. In addition, the investments are relatively high. Nevertheless, this research is highly necessary. In 1999, the European Union adopted a special regulation in order to stimulate the development of new therapies for rare diseases. That policy is yielding positive results.
Companies worldwide are responsible for the vast majority of drug research and development (R&D) investments. They work together with public organisations. Companies account for approximately 73% of the billions invested. Universities and governments account for smaller percentages, 15 and 12, respectively. In total, more than 132 billion euros was involved in 2014.
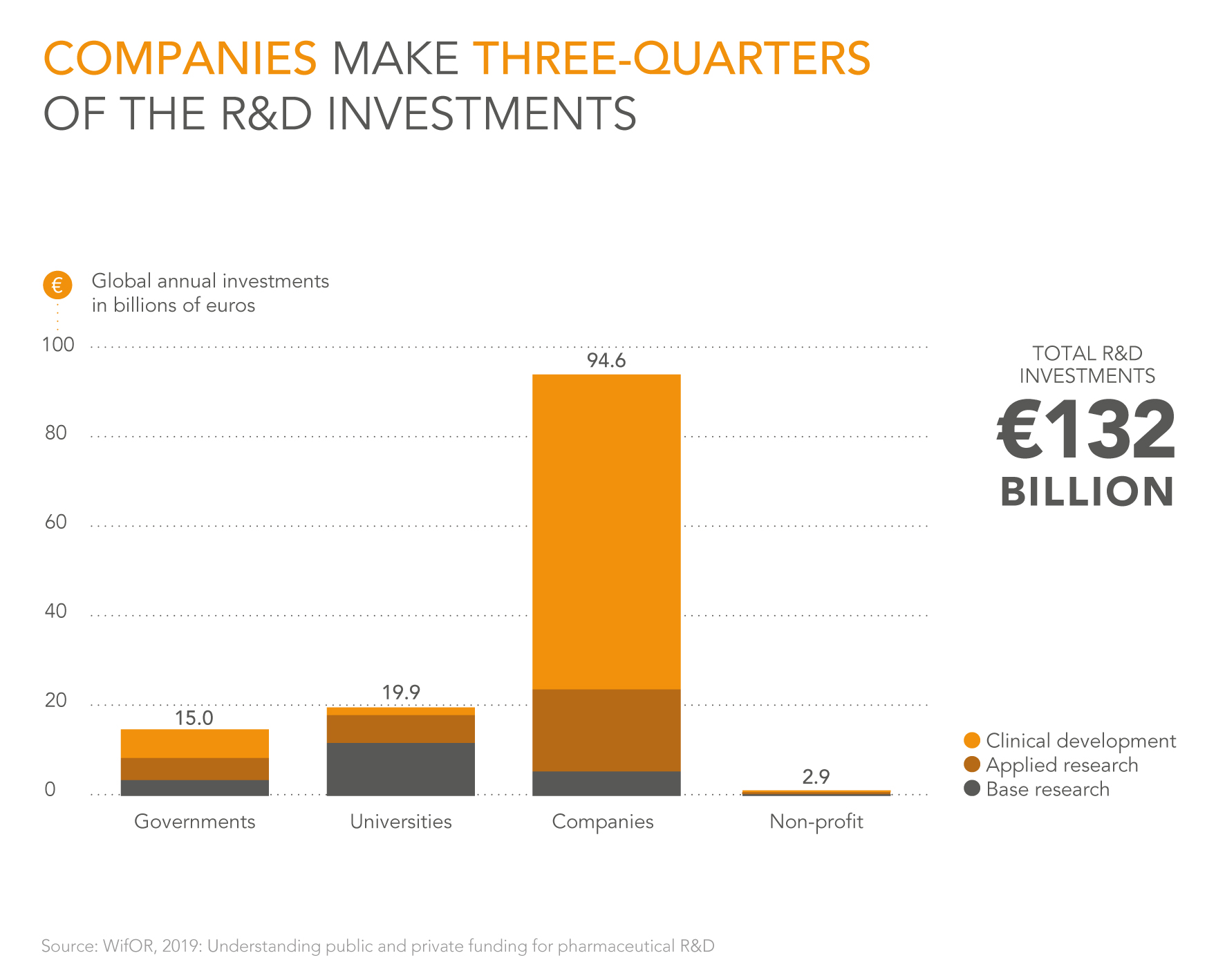
Source: WifOR, 2019: Understanding public and private funding for pharmaceutical R&D
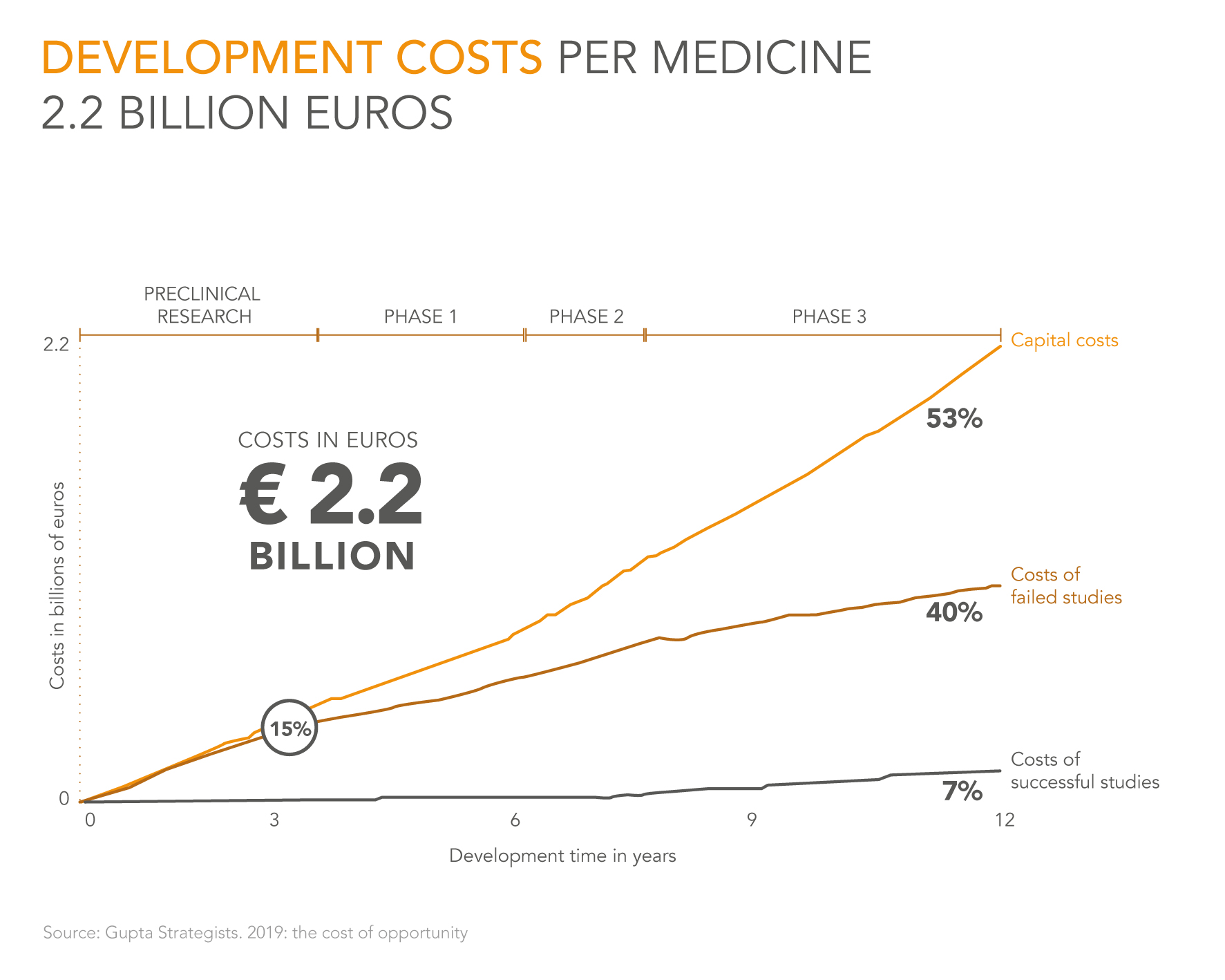
Source: Gupta Strategists, 2019: the cost of opportunity
On average, its costs 2.2 billion euros to develop and test a new drug and bring it to the patient. More than half of these costs are cost of capital. Those costs consist of the return that investors, such as pension funds or healthcare insurers, require for their capital. They expect a higher return if they make their capital available for a longer period of time. That can increase considerably in 10-12 years, the period required for drug development.
The costs of failed research also comprise a large portion of the development costs. That is because the vast majority of drugs do not reach the finish line. Even after the preclinical phase, approximately 89% still drop out.
The best way to restrict development costs is to lower the cost of capital. That can be done, for example, by already providing the new medicine earlier on to a large group of patients. That has another important benefit. It means that more people receive a medicine at an earlier stage, which can have a great effect on the quality of their lives.
The Netherlands has accrued a great deal of knowledge and expertise over a relatively small geographical area in the field of drug development. Consider the universities, the biopharmaceutical companies and the number of clinical studies.
The excellent infrastructure, with examples such as Schiphol and the Port of Rotterdam, but certainly the arrival of the European Medicines Agency in Amsterdam in 2019, makes it even more attractive for drug companies to be located in our country.
PharmInvestHolland, a public-private partnership that also includes the Dutch Association Innovative Medicines, has aspired since 2017 to set up an optimal business environment.
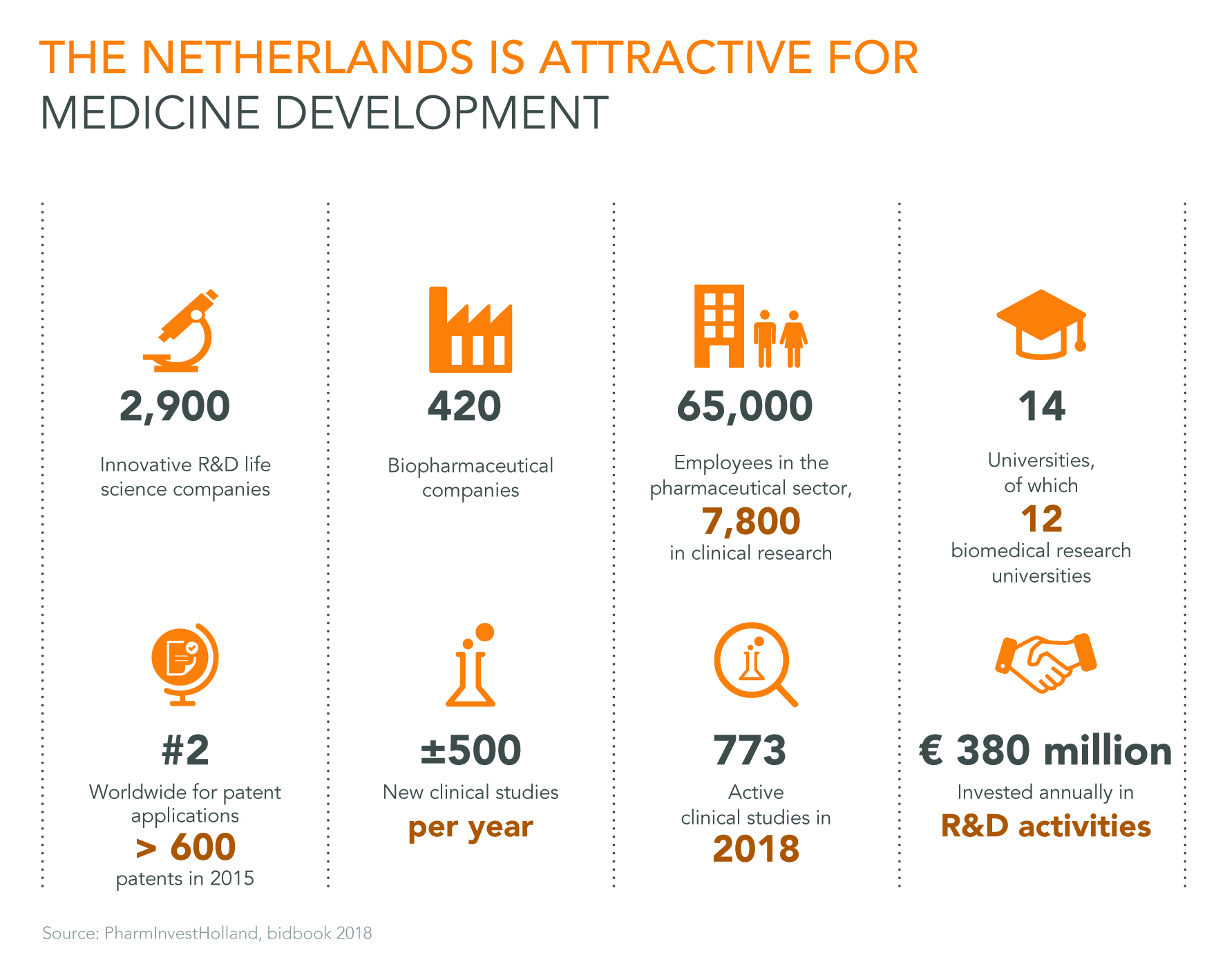
Source: PharmInvestHolland, bidbook 2018

Source: Strategy& 2018: The global innovation 1000 study
In addition to companies such as Amazon, Apple and Samsung, the top 20 companies that invest the most worldwide in research & development include no less than six pharmaceutical companies: Roche, Johnson & Johnson, Merck (known as MSD in Europe), Pfizer, Novartis and Sanfi.
The top 100 of the largest R&D investors include 25 (bio)pharmaceutical companies. Together, they hold more than one-quarter of the investments of the one hundred largest investors.
Pharmaceutical companies therefore make significant investments in R&D, especially in comparison with other industries. In 2018, the 145 largest (bio)pharmaceutical investors invested a total of 131 billion euros. This is good for the patient, the economy and employment. The six pharmaceutical companies that invest the most in R&D spend, on average, more than 17% of their revenue on it.
Patents are at the heart of the innovative pharmaceutical industry. Patents drive innovation in two ways. First, they offer protection for a number of years against duplication of a medicine, giving a drug company a greater chance to recoup their investment. And second, the company can inspire other researchers by making its knowledge public.
Once a potential new drug has been discovered, a patent application is submitted. Starting from that moment, the patent is valid for 20 years. Of those years, 12 years will have already passed when it gets to the patient as a registered drug, due to the years of studies in patients. When the patent has expired, other companies can copy the drug. Then the price of the medicine often decreases significantly. During the entire patent period, companies can, of course, also develop a different medicine for the same disorder. This means that, in reality, the ‘actual’ patent period often lasts only a few years.

Source: Dutch Association Innovative Medicines
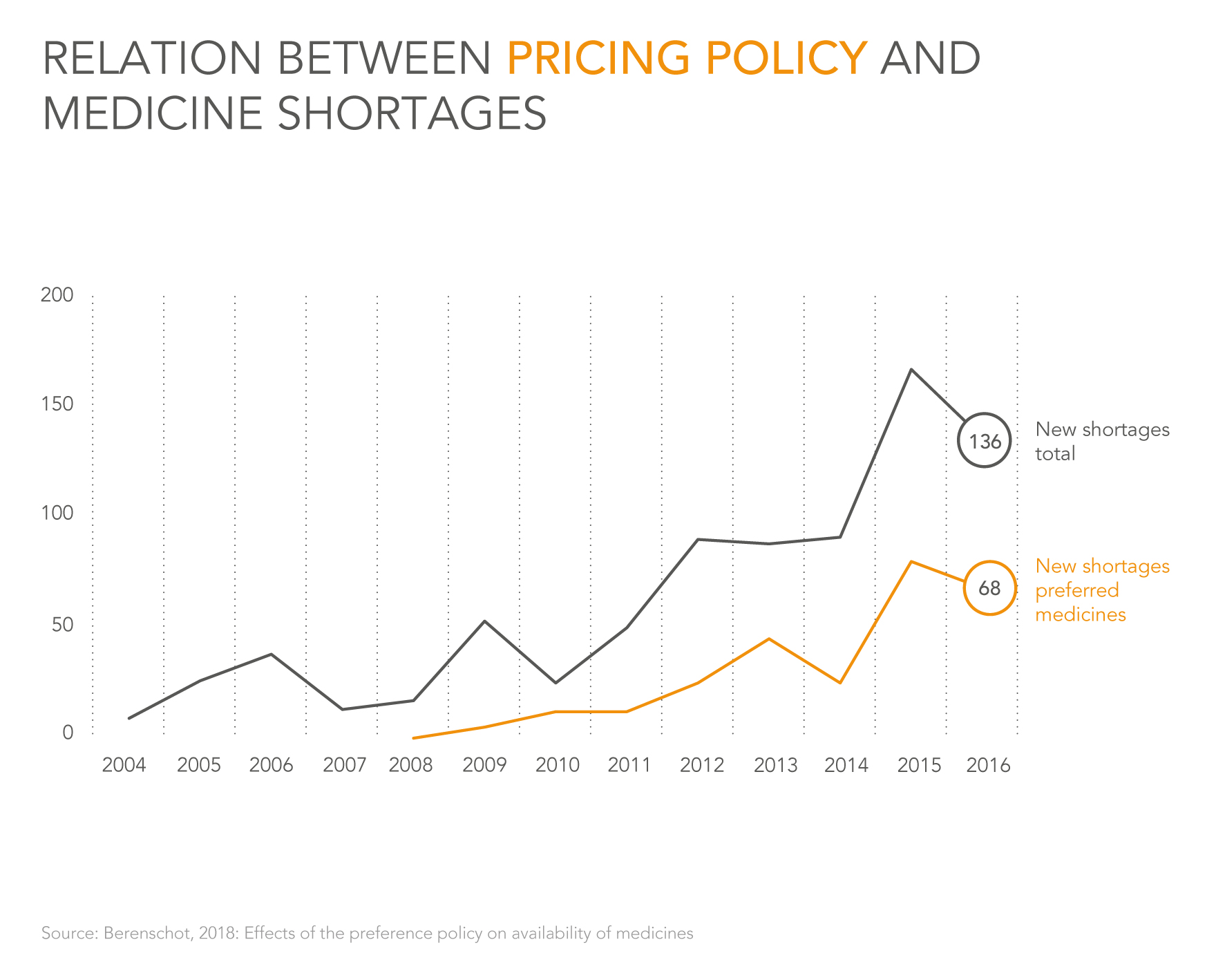
Source: Berenschot, 2018: Effects of the preference policy on availability of medicines
Shortages of medicines are a global problem involving many parties. These can have several causes. For example, there can be problems with the availability of raw materials, or the vulnerable, often complex manufacturing process.
One of the causes is the preference policy that exists in the Netherlands, where only the cheapest medicine for a specific disorder is reimbursed. Since the introduction of this policy, the number of shortages under preferred medicines has increased considerably more than for medicines in general. Therefore, an increasingly greater share of the shortages also involve preferred medicines. Berenschot Consulting Agency concludes from this that there is probably a connection with the preference policy. The Dutch Association Innovative Medicines is actively working on concrete solutions for shortages. In 2019, an independent analysis will begin regarding the structural causes of shortages in the Netherlands and beyond.
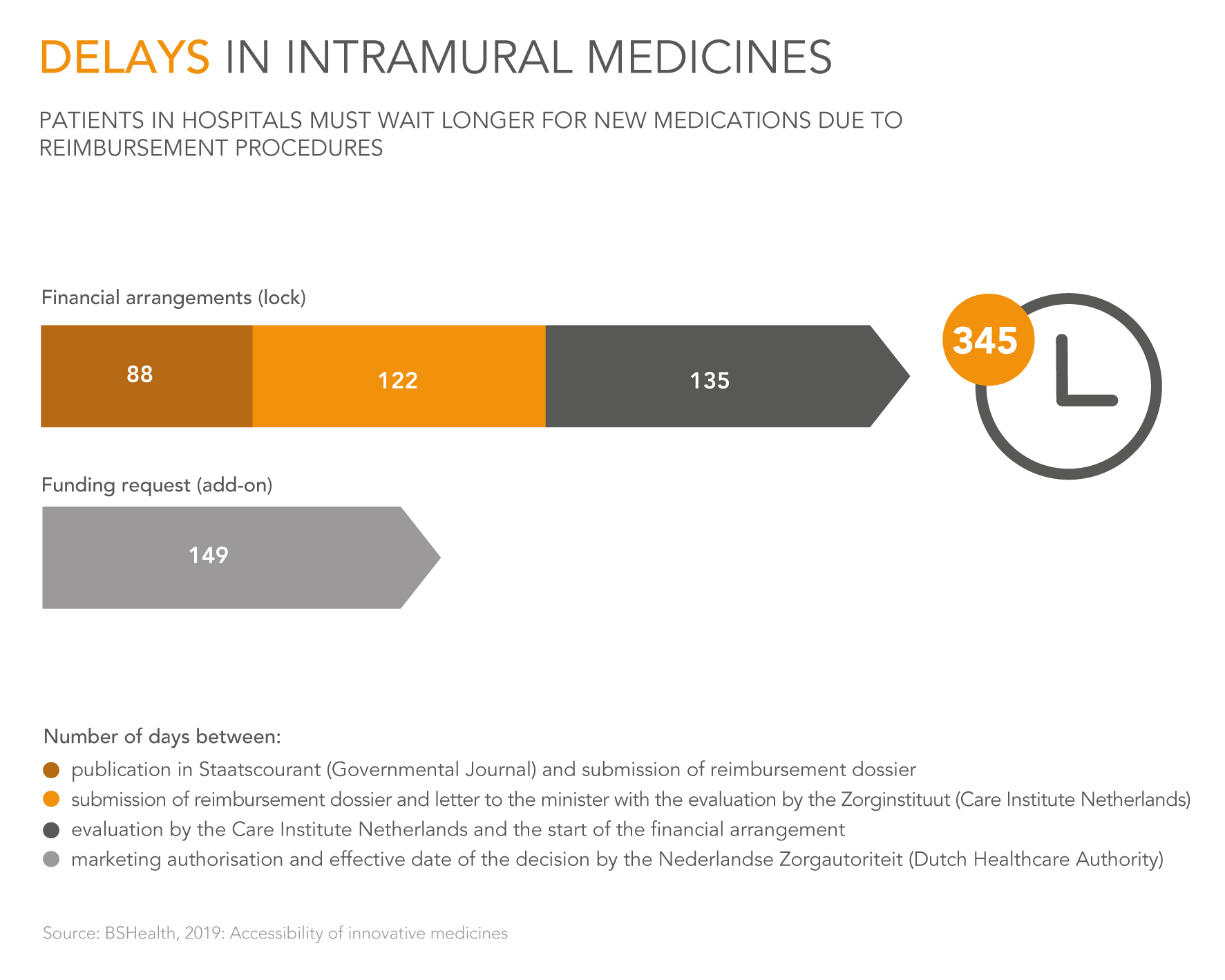
When a new medicine is used in hospitals, it is automatically reimbursed for Dutch patients through their basic health insurance. However, this does not mean that all patients receive the medicine immediately. When a medicine costs society more than 40 million euros per year in total, it is placed in the so-called ‘lock’. This also occurs when the medicine costs more than 50,000 euros per patient and a total of 10 million euros per year. As long as a medicine is in the lock, which is an average of 345 days, it is not available for the patient. The lock often results in a financial arrangement between the government and a pharmaceutical company.
In addition, physicians often only prescribe a medicine when it has separate financing, which is called an ‘add-on’. Even for drugs that have not been placed in the lock, it takes 149 days on average before physicians will prescribe the new medicine.
It is very important to reduce these periods for the patient. For this purpose, consultation is necessary between all involved parties.
Source: BSHealth, 2019: Accessibility of innovative medicines
Source: BSHealth, 2019: Accessibility of innovative medicines
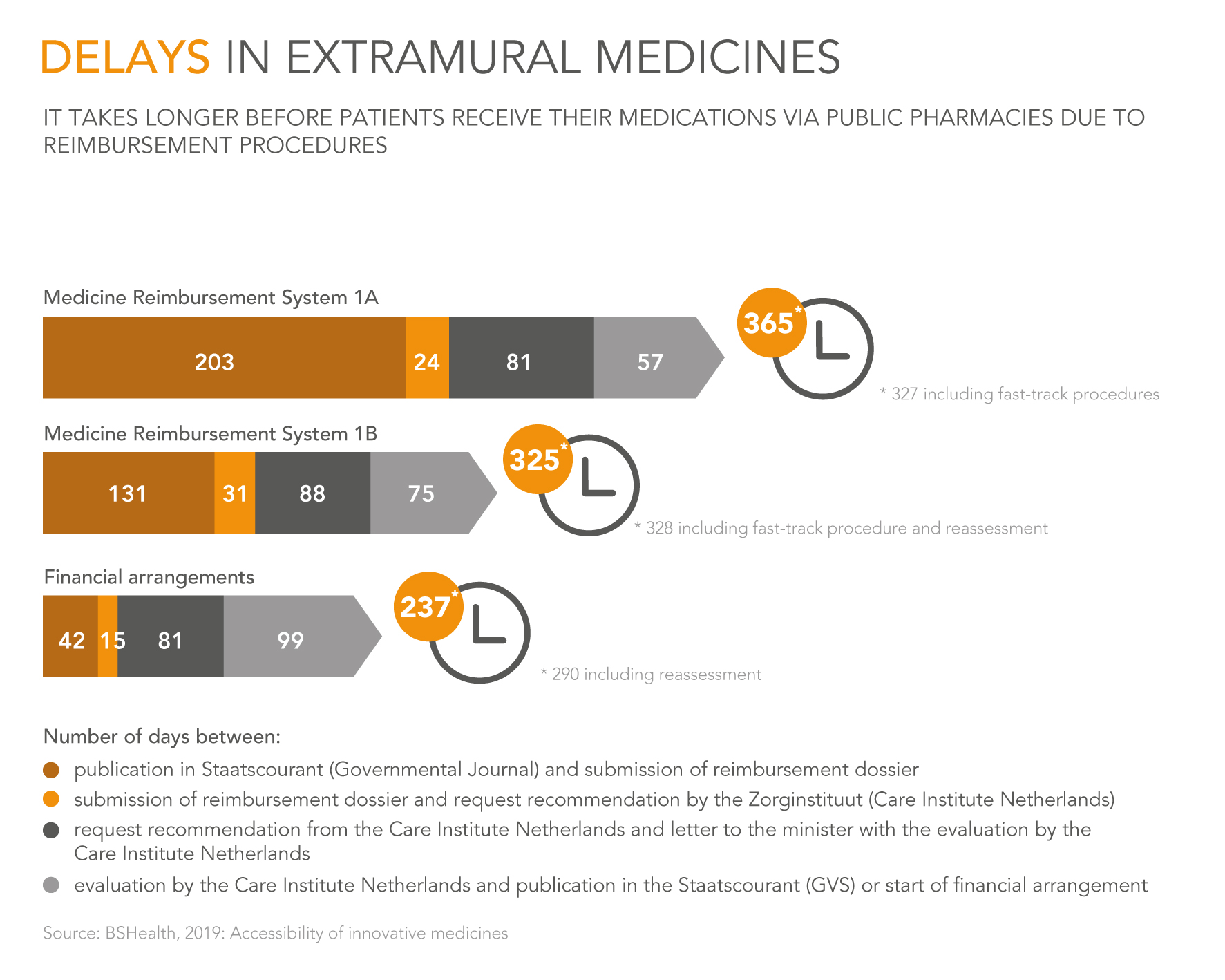
Medicines that get to the patient via the public pharmacy are not automatically reimbursed from the basic health insurance. A drug company must apply for reimbursement through the Geneesmiddelen Vergoeding Systeem (GVS) [Medicines Reimbursement System]. This application is submitted to the Minister of Medical Care, who requests a recommendation from the Zorginstituut (National Healthcare Institute). Based on this recommendation, these medicines will be placed in a cluster with a reimbursement limit (1a) or put on a separate list without limit (1b). These procedures last on average 325 days (1b) and 365 days (1a).
The minister sometimes still negotiates with the drug company about a financial arrangement for expensive medicines. Similar to the lock, this occurs when it the total cost is more than 40 million euros per year or more than 50,000 euros per patient and more than 10 million euros in total. This takes an average of 237 days. Proper consultation is also necessary here in order to be able to help the patient faster.
Google+
Uw naam
Uw e-mail adres
Naam ontvanger
E-mail adres ontvanger
Uw bericht